




 0752-2228195
0752-2228195
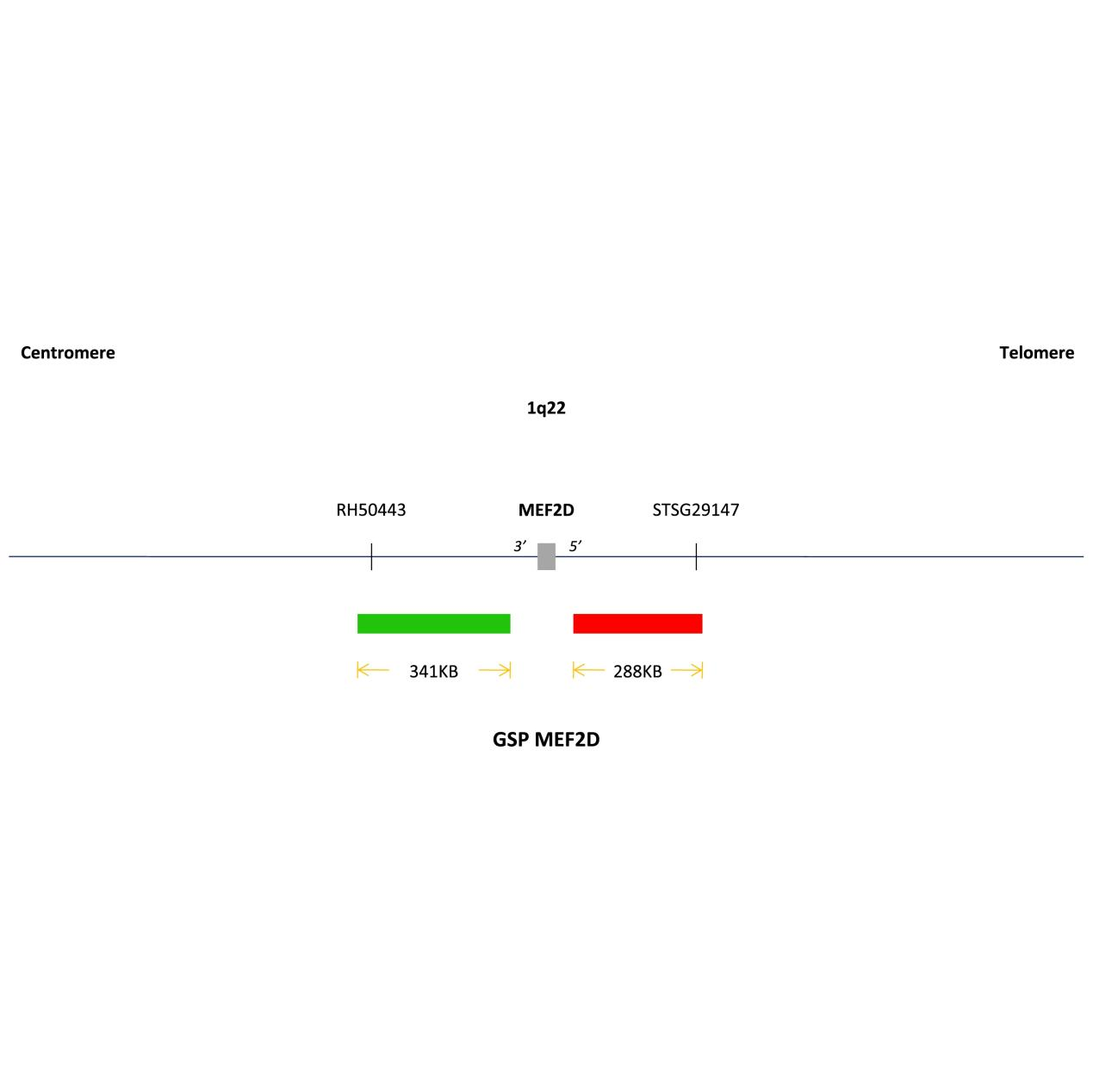
MEF2D (1q22) gene breakage probe reagent
Wholesale Price(RMB):
30006000330066003300660036007200
Product Code:R-0501070Ⅰ-01/R-0501070Ⅰ-02/R-0501070Ⅱ-01/R-0501070Ⅱ-02/R-0501070Ⅲ-01/R-0501070Ⅲ-02/R-0501070Ⅳ-01/R-0501070Ⅳ-02
Probe name:GSP MEF2D(Centromere)/ GSP MEF2D(Telomere)
Product Code:Type I (direct FISH method)/Type II (biotin-labeled indirect FISH method)/Type III (digoxigenin-labeled indirect FISH method)/Type IV (TSA-FISH method)
Product Specifications:
5T/box(Ⅰ-01)10T/box(Ⅰ-02)5T/box(Ⅱ-01)10T/box(Ⅱ-02)5T/box(Ⅲ-01)10T/box(Ⅲ-02)5T/box(Ⅳ-01)10T/box (IV-02)
Registration Number:










